As we move through 2026, the conversation surrounding the National Health Insurance (NHI) has shifted from theoretical debate to a high-stakes legal and operational reality. With the Constitutional Court hearings in May 2026 serving as a pivotal “reset” moment, many South Africans remain caught between political rhetoric and genuine concern for their future medical care.
Understanding how NHI will work in South Africa 2026 requires looking past the headlines to the granular changes in how services are purchased, how doctors are accredited, and how the very definition of “medical aid” is being legally redefined.
Our Selection Methodology
To determine the seven most critical “unknowns,” we analyzed the NHI Act No. 20 of 2023, the 2026 National Budget Review, and the specific litigation papers filed for the May 2026 Constitutional Court session. We prioritized facts that directly impact the average citizen’s “point-of-care” experience and financial planning. Our selection criteria focused on the legal “Complementary Cover” transition, the specific “referral pathway” requirements, and the technical accreditation hurdles for private providers that will define the quality of care in this new landscape.
7 Things Most People Don’t Know About How NHI Will Work In South Africa and Change The Healthcare Landscape for Everyone
The road to universal coverage is more complex than a simple “switch” from private to public; it is a fundamental re-engineering of the entire healthcare economy.
1. The May 2026 Constitutional Court “Pause” is a Structural Reset
While the Act was signed in 2024, the government agreed in early 2026 to delay the proclamation of key sections until the Constitutional Court rules on the public participation process.
-
Best for: Individuals wondering why their medical aid hasn’t changed overnight despite the legislation being “law.”
-
Things to consider: This pause is specifically focused on the legality of the process, meaning a ruling in mid-2026 could either trigger an immediate Phase 2 rollout or send the Act back to Parliament for revision.
This legal bottleneck ensures that while the concept of NHI is fixed, the actual implementation of the fund as a “single purchaser” remains in a state of flux until the judgment is delivered.
2. Medical Aids aren’t Dying—They are Shrinking into “Complementary” Roles
A common myth is that medical aids will be banned; the reality is that once NHI is “fully implemented,” they can only cover what the NHI Fund does not cover.
-
Best for: Current medical scheme members trying to decide whether to cancel their plans.
-
Things to consider: This “Section 33” rule means your medical aid will likely transform into a “top-up” service for luxury wards, non-essential surgeries, or specialized experimental treatments.
The survival of private schemes depends entirely on the “benefit basket” the NHI Fund chooses to prioritize first.
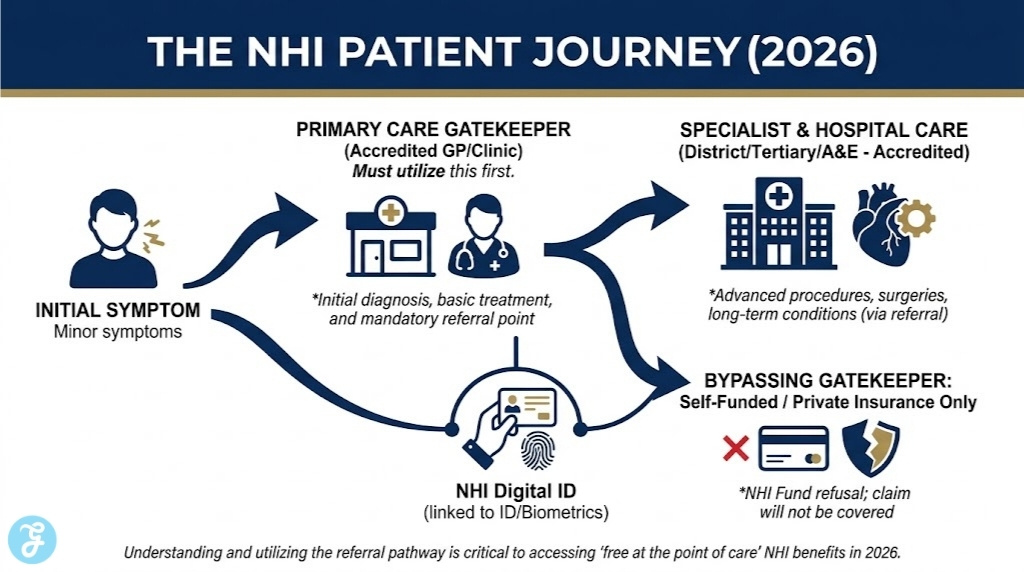
3. The Mandatory “Referral Pathway” Requirement
Under the 2026 framework, the NHI will not pay for your specialist visit or hospital stay if you do not first visit a primary “gatekeeper,” such as a local clinic or GP.
-
Best for: Patients accustomed to booking direct appointments with specialists like dermatologists or cardiologists.
-
Things to consider: If you bypass the referral chain, you will be required to pay for the service out of your own pocket or through separate private insurance, as the NHI Fund will refuse the claim.
This shift is designed to reduce costs by ensuring high-level facilities are only used when absolutely necessary.
4. Private Doctors must “Qualify” for the NHI Fund
Simply being a licensed doctor is not enough to get paid by the NHI; private practices must be accredited by the Office of Health Standards Compliance (OHSC).
-
Best for: Residents who want to keep seeing their current private family doctor under the NHI system.
-
Things to consider: Many smaller private practices may struggle with the administrative and infrastructure costs required to meet the strict OHSC “norms and standards” for 2026.
If your doctor isn’t accredited, you won’t be able to use your NHI benefits at their practice.
5. Funding is a Payroll Matter, Not Just “General Tax”
The 2026 Budget cycle has highlighted that while R9.3 billion is currently allocated for “preparation,” the full scheme will eventually require a dedicated payroll tax.
-
Best for: Employees and employers planning their financial outlook for the late 2020s.
-
Things to consider: The Act allows for “mandatory pre-payment” contributions, which are expected to function similarly to UIF or the Skills Development Levy, deducted directly from your salary.
This means that high earners will likely pay twice—once through personal income tax and again through a specific NHI contribution.
6. Phase 2 (2026–2028) Focuses on “Purchasing”
We have officially entered Phase 2, which is intended to be the “intensive” period where the Fund starts contracting with private hospitals and specialists.
-
Best for: Healthcare professionals and facility owners looking to enter into service-level agreements with the state.
-
Things to consider: This phase is highly dependent on the “Money Bills” that the National Treasury must still pass to authorize the actual flow of funds from the centralized pool.
Phase 2 is where the theoretical “one-payer” system actually meets the reality of the private sector’s fee structures.
7. Digital Registration is the New “Medical Aid Card”
The 2026 rollout emphasizes a “Digital Health Information System” where every citizen’s record is linked to their ID and the NHI Fund.
-
Best for: Citizens who currently lack any form of medical history or insurance documentation.
-
Things to consider: Your access to care will be tied to this digital ID; without being “registered” in the national system, the seamless “free at the point of care” promise cannot be fulfilled.
This biometrically linked system aims to reduce fraud and track patient outcomes across both public and private facilities.
Strategic Analysis
The transition from a fragmented system to a unified NHI Fund creates distinct “winners” and “losers” in terms of immediate access. The table below outlines how NHI will work in South Africa 2026 across different population segments.
| Population Segment | Current Status (Pre-NHI) | NHI 2026 Status (Phase 2) | Long-Term Shift |
| Medical Aid Members | Full private access | Continued private access + NHI Grant | Likely “Complementary” only |
| Public Sector Users | State facility dependence | Improved facility standards (indirect grants) | Access to private providers via NHI |
| Private Providers | Fee-for-service / Medical Aid | Preparation for OHSC Accreditation | State-contracted service providers |
Our Top 3 Picks And Why?
-
The Referral Pathway Rule: This is the most significant behavioral change for the middle class. It completely alters how patients interact with the healthcare system, moving away from “consumer choice” toward a managed “gatekeeper” model.
-
Complementary Cover (Section 33): This is the ultimate structural change. It represents the end of the private medical aid industry as we currently know it, forcing schemes to reinvent themselves as “top-up” insurers.
-
OHSC Accreditation: We chose this because it is the “quality filter.” It ensures that the NHI isn’t just about access, but about forcing all facilities (public and private) to meet a single, high standard of care.
Preparation Checklist
-
[ ] Monitor the May 5-7, 2026 Constitutional Court judgment for any changes to the rollout timeline.
-
[ ] Verify if your current GP or local clinic is undergoing OHSC accreditation for NHI contracting.
-
[ ] Review your medical aid’s “Gap Cover” and “Complementary” product offerings for 2027.
-
[ ] Ensure your dependents have valid, biometrically linked IDs for the upcoming digital health registration.
-
[ ] Audit your household budget for potential payroll tax adjustments as the “Money Bills” progress through Parliament.
The Horizon of a Unified Healthcare Future
The move toward National Health Insurance in 2026 is an ambitious attempt to bridge one of the world’s most unequal healthcare divides. While the “single-payer” model promise of “free healthcare for all” is the goal, the reality of how NHI will work in South Africa 2026 is currently a period of rigorous preparation, legal scrutiny, and systemic strengthening.
For the average citizen, the immediate priority is understanding the new “rules of the road”—the referral chains, the accreditation of their favorite doctors, and the changing role of their medical aid. The journey is long, but the milestones of 2026 have set the stage for a healthcare landscape that will look fundamentally different by the end of the decade.
FAQs
-
Will I have to pay when I visit a doctor under NHI? No, the goal is “free at the point of care.” The doctor will bill the NHI Fund directly, provided they are accredited and you have a valid referral.
-
Can I choose any hospital once NHI is active? You will be able to choose from a list of “accredited” providers within your district, but you must follow the referral pathway to ensure the Fund covers the cost.
-
Is the government going to “take” my medical aid savings? No, the funds in your medical aid are private. However, the legislation will eventually limit what your medical aid can offer as a service.