The wall between your thoughts and your muscles has finally crumbled. For centuries, we treated Parkinson’s as a simple mechanical failure of the body, but the discovery of the SCAN brain network Parkinson’s connection proves it’s a glitch in the very soul of how we move. If we don’t recalibrate to precision neurology now, we aren’t just failing 25 million people, we are ignoring the most significant evolution in human biology since the map of the genome.
The Great Medical Lie
For as long as modern medicine has existed, we have been told a fairy tale: that the mind and the body live in different zip codes. If you had a “movement” problem, you went to a neurologist. If you had a “thinking” or “mood” problem, you went to a psychiatrist. This divide wasn’t just a matter of professional convenience; it was a fundamental misunderstanding of what it means to be human.
We treated the brain’s motor cortex like a keyboard. Press the “A” key, and the left pinky moves. Press the “B” key, and the right foot taps. It was neat, organized, and, as we confirmed through the landmark Nature study published in February 2026, completely wrong.
The discovery of the Somato-Cognitive Action Network (SCAN), published in Nature, is the final nail in the coffin of Cartesian dualism. Researchers from the Changping Laboratory and Washington University have found the “bridge.” The SCAN is an interdigitated network within the motor cortex that acts as an integrated circuit that connects your plans, your internal organs, and your physical actions into one seamless loop.
This isn’t just a “new discovery.” It’s a total rewrite of medical history. And if you think this is just about tremors and dopamine, you’re missing the forest for the trees.
Parkinson’s Is Not a Motor Disease
We need to stop calling Parkinson’s a movement disorder. That label is a relic of the 20th century. When we look at the 2026 data, it becomes clear: Parkinson’s is a SCAN disorder.
In a healthy person, the SCAN functions like a high-speed fiber-optic cable, translating the “thought” of standing up into the “act” of movement while simultaneously adjusting your heart rate and blood pressure so you don’t faint. In a Parkinson’s patient, the SCAN exhibits pathological hyperconnectivity to subcortical structures like the thalamus and the basal ganglia. The signals aren’t lost; they are screaming at each other. The brain gets “stuck” because the bridge is overcrowded with noisy data. This is why a patient can “want” to walk but find their feet frozen to the floor. The “mind” is ready, but the “bridge” (the SCAN) is blocked.
The New Map of the Human Machine
| Feature | The Old “Homunculus” Map (Pre-2023) | The New “SCAN” Reality (2026) |
| Philosophy | Mind and Body are separate entities. | Mind and Body are an integrated circuit. |
| Movement | Controlled by specific, isolated brain “slots.” | Controlled by an integrated “action” network. |
| Parkinson’s Root | Deep brain dopamine depletion only. | Hyperconnectivity in the SCAN bridge. |
| Treatment | Chemical “sledgehammers” (Levodopa). | Precision “tuning” (Personalized TMS). |
The Economic and Geopolitical Time Bomb
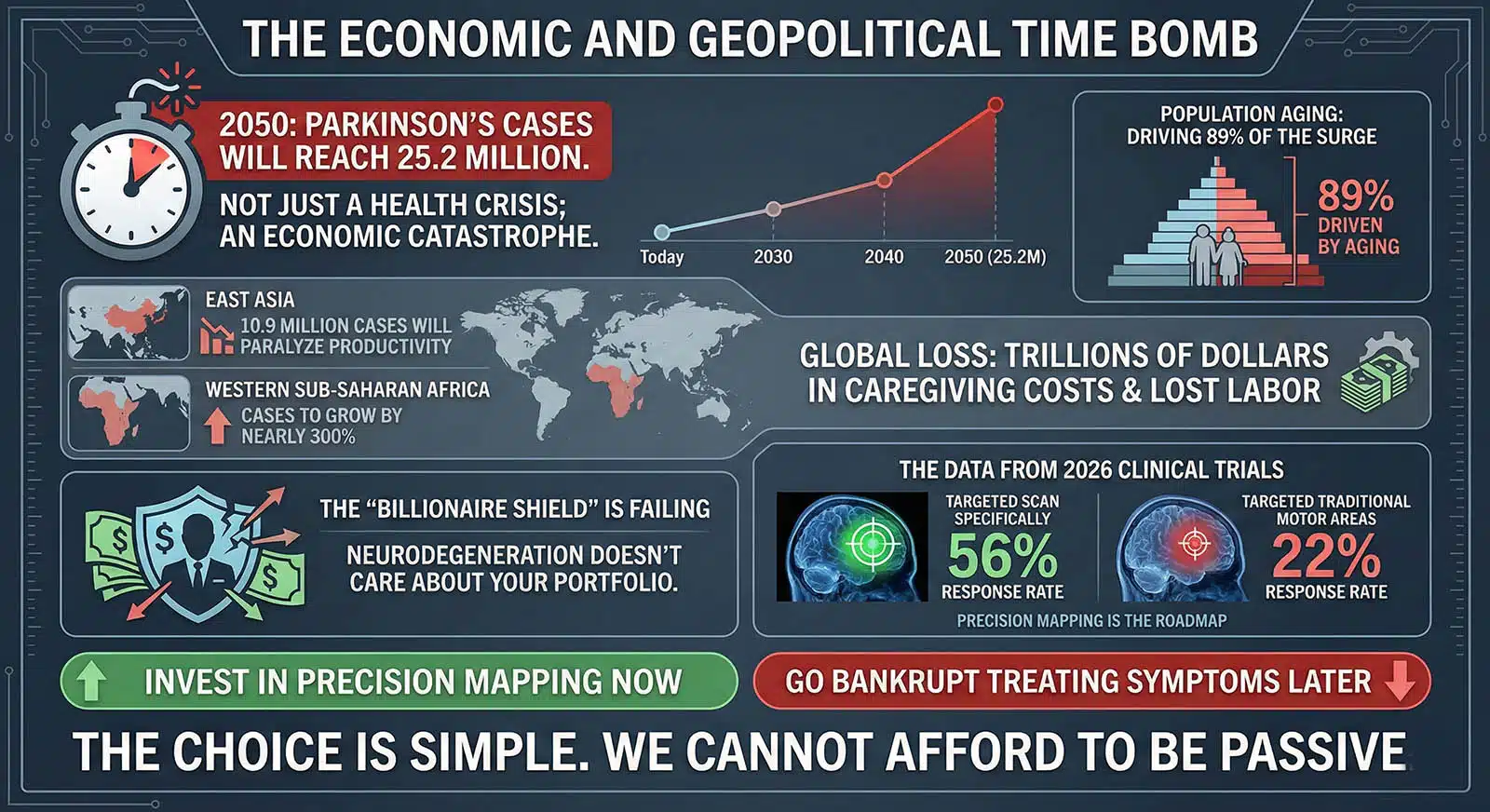
We cannot afford to be passive. By 2050, the number of Parkinson’s cases will reach 25.2 million. This isn’t just a health crisis; it’s an economic catastrophe in the making.
Population aging is driving 89% of this surge. In East Asia, where the workforce is already shrinking, 10.9 million cases will paralyze productivity. In Western Sub-Saharan Africa, cases are set to grow by nearly 300%. We are looking at a global loss of trillions of dollars in caregiving costs and lost labour.
The “Billionaire Shield”, the idea that the elite can buy their way out of aging, is failing. Neurodegeneration doesn’t care about your portfolio. However, the data from the 2026 clinical trials offers a concrete roadmap. When we targeted the SCAN specifically, the response rate was 56%. When we targeted traditional motor areas, it was 22%.
The choice is simple: We either invest in precision mapping now, or we go bankrupt treating symptoms later.
The Counter-Punch: Why “Standard Care” Is Now Malpractice
There are those within the pharmaceutical establishment who argue we should stick to the “gold standard” of Levodopa and traditional DBS. They claim “precision mapping” is a luxury… too expensive and complex for the masses. This is a dangerous fallacy.
They are wrong. Relying solely on systemic drugs in 2026 is like trying to fix a specific software bug by pouring coffee on the motherboard. We now have precision tools, such as low-intensity focused ultrasound and targeted TMS, that bypass systemic distribution entirely.
The argument that precision neurology is “too expensive” fails when you look at the 2026 cost-benefit analysis. A non-invasive TMS session that keeps a patient in the workforce for five more years costs a fraction of a single year in a long-term care facility. To ignore the SCAN is not “conservative” medicine; it is fiscal and moral negligence. The “too expensive” argument collapses under the 2026 cost-benefit analysis. A non-invasive TMS session that keeps a patient in the workforce for five more years costs a fraction of a single year in a long-term care facility. To ignore the SCAN is no longer “conservative” medicine; it is fiscal and moral negligence.
The Moral Imperative: A Roadmap for Change
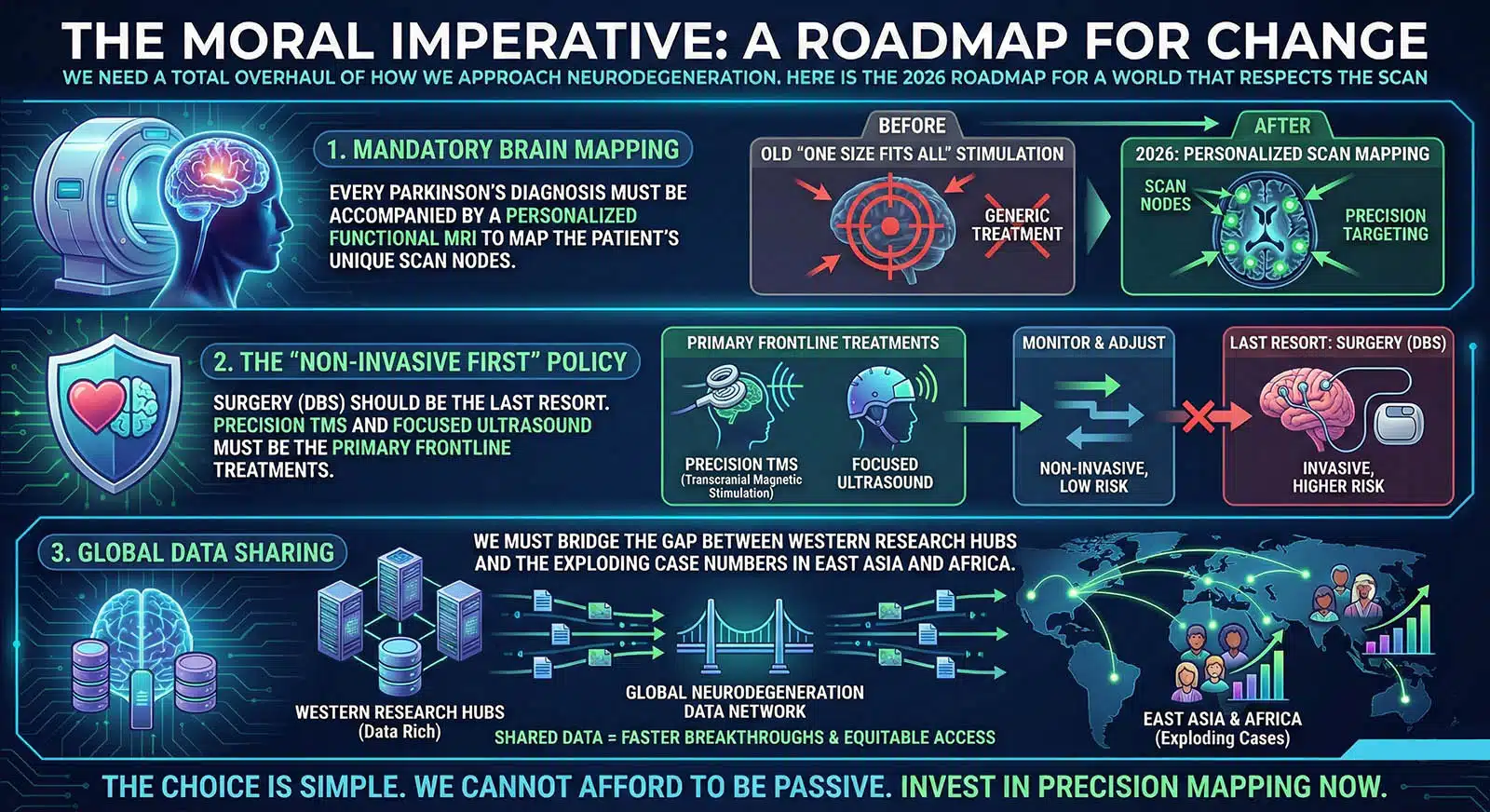
We need a total overhaul of how we approach neurodegeneration. Here is the 2026 roadmap for a world that respects the SCAN:
- Mandatory Brain Mapping: Every Parkinson’s diagnosis must be accompanied by a personalized functional MRI to map the patient’s unique SCAN nodes. No more “one size fits all” stimulation.
- The “Non-Invasive First” Policy: Surgery (DBS) should be the last resort. Precision TMS and focused ultrasound must be the primary frontline treatments.
- Global Data Sharing: We must bridge the gap between Western research hubs and the exploding case numbers in East Asia and Africa.
2026 Fact Sheet: The State of the SCAN
- Response Rate: 56% for SCAN-targeted therapy vs. 22% for traditional targets.
- Global Projection: 25.2 million cases by 2050 (a 112% increase).
- Research Leaders: China (Changping Lab) and the USA (Washington University).
- Technological Shift: 2026 marks the first year non-invasive neuromodulation outperformed systemic drug therapy in clinical response speed.
The Biological Cost of Static Mapping
For decades, we treated the brain as if it were a fixed circuit board. We assumed the motor cortex was an unchanging map of “slots” for fingers, toes, and tongues. The SCAN discovery proves that the brain is far more fluid and integrated than our 20th-century models suggested.
In a Parkinson’s brain, the issue isn’t just that dopamine is missing; it’s that the SCAN has become pathologically rigid. The “inter-effector” nodes, the parts of the network that should coordinate movement with internal physiological states are essentially locked in a feedback loop of high-frequency noise. This is why a patient may experience “freezing of gait” while their heart rate spikes; the coordination between the intent to move and the body’s preparation for that movement has been severed at the network level.
Traditional treatments like Levodopa attempt to fix this by flooding the entire system with chemicals. It is a “shotgun” approach to a “sniper” problem. The 2026 data shows that when we use precision neuromodulation to specifically dampen this SCAN hyperconnectivity, we aren’t just masking a tremor. We are restoring the natural flexibility of the human motor system. This shift from “replacement therapy” to “network tuning” is the difference between keeping a patient dependent on pills and returning them to a state of functional autonomy.
The Geopolitical Imperative for Precision
The explosion of Parkinson’s cases is no longer a distant threat; it is a current reality. By 2050, the global patient population will hit 25.2 million, with the most aggressive growth occurring in regions currently least equipped to handle it. In East Asia, the intersection of a shrinking workforce and a doubling of neurodegenerative cases creates a “productivity trap” that could destabilize local economies. In Western Sub-Saharan Africa, where cases are projected to rise by nearly 300%, the infrastructure for traditional, long-term chronic care simply does not exist.
This is why the push for non-invasive, SCAN-targeted therapies is a geopolitical necessity. We cannot build enough nursing homes to house 25 million people, but we can deploy portable, precision neuromodulation technology. The 2026 breakthrough provides the first scalable solution to this crisis. Because SCAN-targeted TMS is non-invasive and increasingly automated, it can be deployed in regions without a high density of neurosurgeons. This “democratization of neurology” is the only way to prevent a global caregiving collapse.
The Context vs. The Conviction
Context: We found a new network called the SCAN. It connects thinking to moving. Parkinson’s patients have too much activity there.
Opinion: The discovery of the SCAN is the death of “General Neurology.” From this moment forward, any doctor who treats a Parkinson’s patient without first mapping their SCAN network is practicing 19th-century medicine in a 21st-century world. We have finally found the bridge between our intentions and our actions. To leave it broken when we have the tools to fix it is a betrayal of the millions who are currently “frozen” in their own bodies.
What Happens Next?
In the next 24 months, expect to see a surge in “Neuromodulation Clinics” that look more like high-tech spas than hospitals. We will see the first FDA-approved wearable “SCAN-tuners,” headsets that use low-intensity signals to keep the bridge clear throughout the day.
But here is the final question: Now that we know the mind and body are one, are we brave enough to stop treating the symptoms of the machine and start healing the connectivity of the human?