The landmark passage of the Mental Health Act 2025 has initiated a transformative era for psychiatric services in England and Wales. As the healthcare sector moves into the 2026 implementation phase, the focus has shifted from a system of custodial oversight to one grounded in the four core principles: choice and autonomy, least restriction, therapeutic benefit, and the person as an individual. These reforms aim to modernise a framework that has remained largely unchanged since 1983, ensuring that the Mental Health Act Reform UK delivers a more humane and effective standard of care.
How We Selected Our 7 Proven Ways the UK’s Mental Health Act Reform Will Change Psychiatric Care
To identify the most impactful changes, we analysed the final statutory text of the 2025 Act, the NHS England implementation roadmap for 2026, and the latest consultation drafts for the new Code of Practice. The following criteria were used to ensure the most relevant updates were highlighted for stakeholders.
Our selection was filtered based on the immediate legal impact on detention criteria, the shift in patient representation rights, and the statutory requirements for clinical documentation. These seven points represent the gold standard of the reform’s promise to reduce inappropriate detention and empower service users.
The 7 Most Significant Impacts of the Mental Health Act Reform UK
The 2026 implementation represents a paradigm shift in how clinicians, patients, and families interact within the psychiatric system. Each of these changes is designed to ensure that detention is a last resort and that every hour spent in hospital is focused on a clear path to recovery and discharge.
1. The Introduction of the “Serious Harm” Detention Threshold
The most fundamental change to the Mental Health Act Reform UK is the heightening of the criteria for detention. Under the old rules, a general risk of harm was often sufficient to justify a loss of liberty.
Best for: Clinicians and Approved Mental Health Professionals who must now provide more robust justifications for Section 2 and Section 3 admissions.
Why We Chose It:
-
It directly addresses the principle of least restriction by raising the legal bar for detention.
-
It requires a more sophisticated clinical assessment of risk, moving away from vague safety concerns.
-
It aligns UK law with international human rights standards regarding the right to liberty.
Things to consider: The new Code of Practice will provide the granular definition of what constitutes serious versus significant harm during the upcoming 2026 review cycles.
2. Ending Section 3 Detention for Learning Disabilities and Autism
A landmark victory for neurodiversity advocates, the 2025 Act clarifies the status of neurodivergent individuals within the healthcare system. This ensures that hospitals are used for medical treatment rather than social containment.
Best for: Autistic individuals and those with learning disabilities who have historically been stuck in inappropriate inpatient settings for years.
Why We Chose It:
-
It ends the revolving door of hospitalisation for people who actually require community-based social support.
-
It forces local authorities and Integrated Care Boards to invest in community crisis housing and specialist support teams.
-
It recognises that neurodivergence is a lifelong difference, not a condition to be cured in a psychiatric ward.
Things to consider: This change does not apply to individuals entering the system via the criminal justice route where separate forensic safeguards apply.
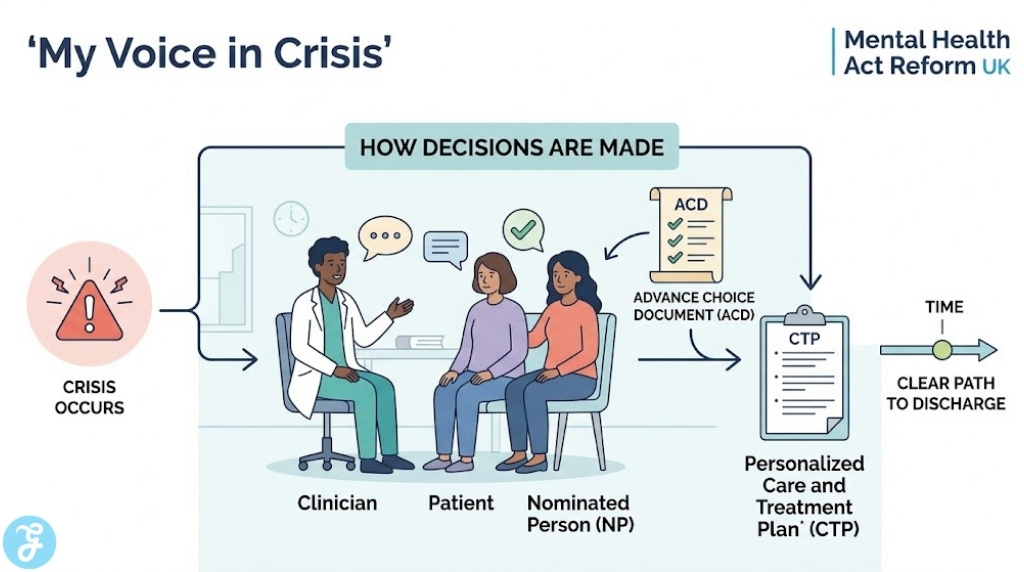
3. Mandatory Statutory Care and Treatment Plans (CTPs)
For the first time in English law, every patient detained under the Act must have a statutory Care and Treatment Plan. This legal requirement ensures that no patient is left without a clear clinical direction.
Best for: Patients and their families who have previously felt lost in the system without a clear end date or treatment goal.
Why We Chose It:
-
It holds clinical teams accountable for providing active, beneficial treatment rather than just containment.
-
It ensures that the patient’s voice and the voice of their carers is documented within the legal record of their care.
-
It standardises the quality of care planning across all NHS and private providers.
Things to consider: If a CTP is not updated or does not demonstrate a clear therapeutic benefit, it can be used as strong evidence during a Mental Health Tribunal to argue for discharge.
4. Replacing the “Nearest Relative” with a “Nominated Person”
The outdated and rigid hierarchy of the Nearest Relative has been abolished to better reflect modern family structures. Patients now have the power to choose their own representatives instead of relying on a legal default.
Best for: LGBTQ+ individuals, those with complex family dynamics, or anyone who prefers a trusted friend over a biological relative.
Why We Chose It:
-
It significantly enhances patient autonomy and the right to a private and family life.
-
It grants the Nominated Person new rights, such as the power to object to a Community Treatment Order.
-
It ensures that the person most familiar with the patient’s wishes is legally involved in the decision-making process.
Things to consider: If a patient lacks the capacity to choose a Nominated Person, the court can appoint one who is best suited to represent the patient’s interests.
5. Statutory Weight for Advance Choice Documents (ACDs)
Advance Choice Documents allow individuals to document their treatment preferences and preferred medications while they are well. This gives patients a voice even during their most vulnerable moments in a crisis.
Best for: Individuals with fluctuating conditions, such as Bipolar Disorder or Psychosis, who want to maintain control over their future crisis care.
Why We Chose It:
-
It provides a proactive way to manage mental health crises and reduces the trauma of forced treatment.
-
It ensures that past expert experience of what works for the patient is respected by new clinical teams.
-
It promotes the person-centred care model that is central to modern psychiatry.
Things to consider: While not 100% legally binding, the requirement for a compelling reason to ignore an ACD is a high hurdle for clinicians.
6. Accelerated Access to Mental Health Tribunals
Waiting six months for a chance to challenge a Section 3 detention is no longer the standard under the 2026 guidelines. Patients now have more frequent opportunities to seek independent judicial review.
Best for: Detained patients who feel they are well enough to go home and want an independent legal review of their case.
Why We Chose It:
-
It provides a vital safeguard against unnecessary or over-extended detention.
-
It increases the judicial oversight of the psychiatric system.
-
It ensures that the serious harm and therapeutic benefit tests are being met on a continuous basis.
Things to consider: More frequent tribunals mean that patients will need more consistent access to Independent Mental Health Advocates which the 2026 reform also expands.
7. Ending the Use of Police and Prison Cells as “Places of Safety”
The 2025 Act has finally closed the loophole that allowed individuals in a mental health crisis to be held in criminal justice settings. A mental health crisis is now legally recognized as a medical emergency.
Best for: Vulnerable individuals in crisis who have historically been traumatised by being placed in a cell during their most difficult moments.
Why We Chose It:
-
It removes the stigma of criminalising mental illness.
-
It ensures that the very first point of contact in a crisis is with clinical staff, not just the police.
-
It sets a clear 28 day limit for the transfer of prisoners to mental health hospitals if they require acute care.
Things to consider: This change places significant pressure on the NHS to ensure that S136 suites and crisis hubs are adequately staffed and available 24/7.
Comparing the Pre-Reform and 2026 Psychiatric Care Models
The impact of the Mental Health Act Reform UK is best understood by looking at the specific legal shifts in how patients move through the system. The transition from the legacy framework to the modernised 2026 standards focuses on human rights and clinical efficacy.
The table below provides a high-level summary of the structural changes between the old Act and the new 2025 legislation being implemented this year.
| Feature | Legacy Model (MHA 1983) | Reform Model (MHA 2025/26) |
| Detention Threshold | Vague risk of harm | Stricter Serious Harm test |
| Neurodivergence | LD/Autism detenable | LD/Autism excluded from Section 3 |
| Care Planning | Discretionary care plans | Mandatory Statutory CTPs |
| Patient Representation | Nearest Relative (Fixed) | Nominated Person (Chosen) |
| Advance Wishes | Informally considered | Statutory Advance Choice Docs |
| Places of Safety | Police cells permitted | Healthcare facilities only |
Our Top 3 Picks and Why?
Of the seven ways identified, the Serious Harm Threshold, the Nominated Person, and Advance Choice Documents are the most transformative. These updates represent the core of the 2026 paradigm shift.
These three changes fundamentally shift the power dynamic in psychiatric care. They move the burden of proof onto the state to justify detention, return the right to choose representatives to the patient, and ensure that a person’s expert knowledge of their own illness is legally respected even during a crisis.
Adapting to these changes requires a proactive approach, whether you are a service user, a family member, or a legal professional. Understanding the new statutory rights is the first step toward better outcomes in a psychiatric setting.
The Selection Framework:
-
For Service Users: Create your Advance Choice Document and name your Nominated Person while you are well. This ensures your preferences are locked in legally.
-
For Families: Familiarise yourself with the new rights of the Nominated Person, specifically the ability to object to treatment orders.
-
For Clinicians: Standardise your reporting to include specific evidence for the Serious Harm test and ensure every CTP has a discharge-focused goal.
Decision Matrix (Table):
The following matrix provides guidance on which protective measures to prioritise based on your specific needs within the new legal framework.
| If you want to… | Then you should… |
| Control who receives your clinical updates. | Designate a Nominated Person formally. |
| Prevent a specific medication from being used. | Outline this in an Advance Choice Document. |
| Challenge a long-term Section 3 detention. | Apply for a Mental Health Tribunal every 3 months. |
The Final Checklist: 5-point Readiness for Mental Health Reform
Before the full implementation reaches its next phase, ensure you have completed these critical steps to safeguard patient rights. Proactive preparation is the key to navigating the new legal landscape.
-
Have you officially named your Nominated Person and informed them of their role?
-
Do you have a physical and digital copy of your Advance Choice Document ready?
-
If currently detained, have you asked for a copy of your Statutory Care and Treatment Plan?
-
Have you verified that your local crisis hub is a designated Place of Safety?
-
Are you aware of the new shortened review windows for challenging Section 3?
The Future of Psychiatric Justice in the UK
The 2026 implementation of the Mental Health Act Reform UK is more than just a legislative update; it is a cultural shift. By embedding the principles of choice and therapeutic benefit into the heart of the law, the UK has set a new global benchmark for psychiatric care. While the full transition will take time, the proven ways listed above are already beginning to change the lives of thousands, ensuring that mental health care is defined by dignity rather than detention.