The room in Ghaziabad is painfully quiet. A rhythmic, mechanical hum from a feeding machine fills the silence. Harish Rana lay in a bed exactly like this for 13 years. In 2013, a devastating fall from a fourth floor balcony in Chandigarh broke his body and abruptly ended his promising journey as a young engineering student. He suffered complete quadriplegia. As we examine euthanasia laws by country 2026, this case illustrates how a body can survive an initial physical impact without truly waking up again.
The Supreme Court of India describes this permanent vegetative state as wakefulness without awareness. It is a haunting medical reality. His eyes would open and close with the passing of day and night. The body sleeps and wakes in a simulated rhythm. Yet, the self inside is entirely absent. There is no cognitive recognition. There is no communication. There is only a physical shell sustained by electricity and clinical formulas.
The March 11 Supreme Court verdict in India offers a profound global lesson in mercy. The international conversation around the right to die often becomes entangled in complex, abstract legal theory. The Harish Rana ruling strips away the bureaucracy and forces us to look directly at the devastating human cost.
This tragedy introduces a concept we might call the Biological Mirror. Modern medicine possesses an incredible, almost miraculous ability to preserve life. Doctors can keep a heart beating, lungs expanding, and blood circulating indefinitely. However, this technology sometimes ends up reflecting only the grief of the living. Medical machines keep biological functions running smoothly, while the actual person departed over a decade ago. It creates a terrifying twilight zone for families. Parents watch their loved one breathe, but they cannot reach him. In its relentless quest to defeat death, medicine sometimes creates a prison of prolonged biological existence.
From Legal Limbo to Human Experience
For years, Harish and his family were trapped in this medical purgatory. India formally recognised the right to die with dignity on paper during a landmark ruling in 2018. However, that legal theory remained entirely disconnected from the grim reality of hospital wards. The March 2026 verdict changed everything.
Justices J.B. Pardiwala and K.V. Viswanathan delivered a historic judgement. They finally moved the nation from abstract constitutional guidelines to human reality. They formally recognised that a feeding tube is a complex medical intervention, not merely a provision of basic care. By allowing the withdrawal of clinically assisted nutrition, the highest court made a definitive, compassionate statement: true care sometimes means having the absolute courage to let go.
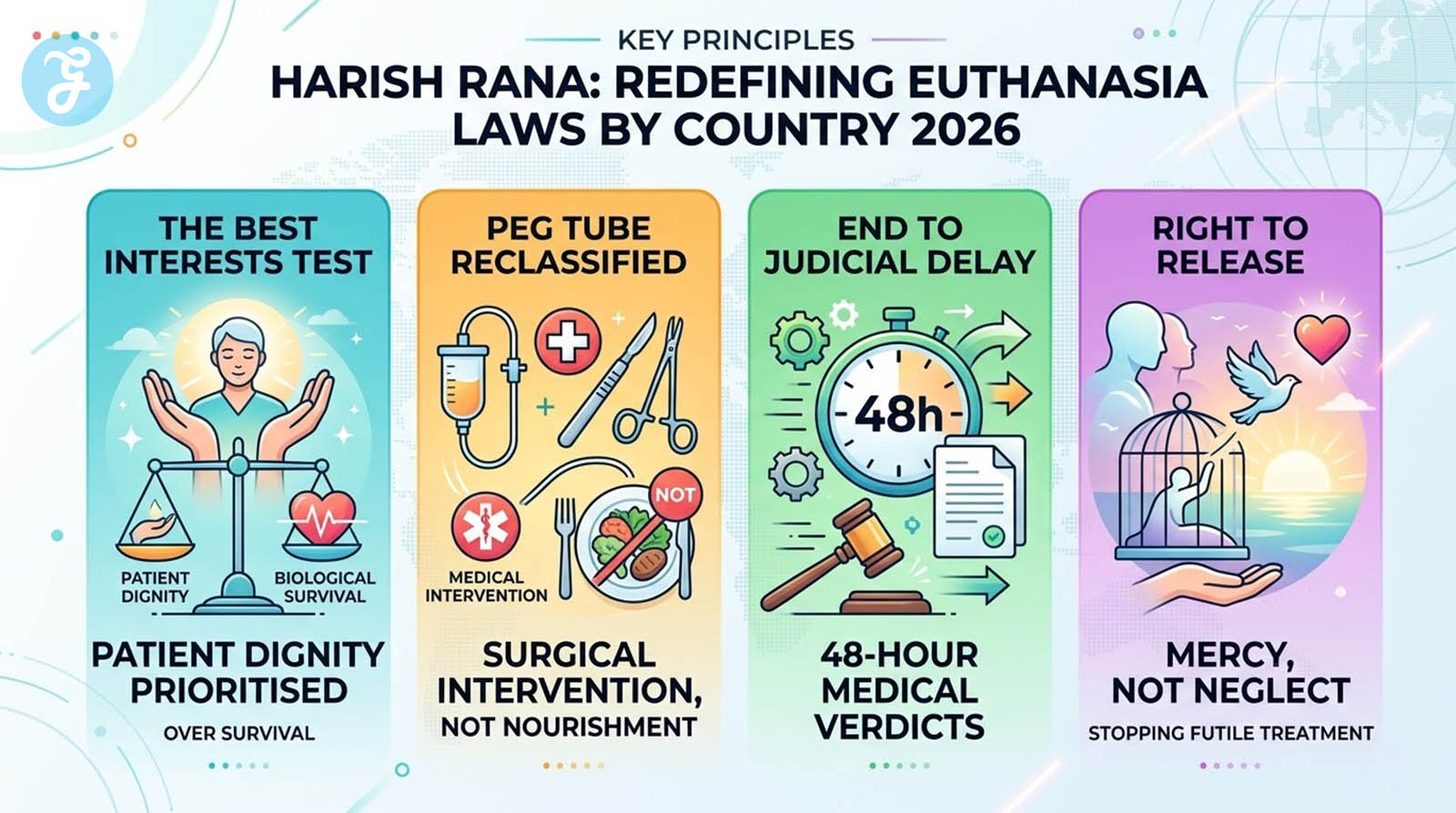
Harish Rana: Redefining Euthanasia Laws by Country 2026
Following his catastrophic fall in 2013, Harish spent over a decade trapped in a permanent vegetative state. After enduring years of emotional and financial exhaustion, his parents approached the courts to stop this endless medical loop. The Delhi High Court firmly rejected their plea in 2024. The lower court judges feared that withdrawing support essentially equated to starvation. They viewed stopping hydration as an unnatural act of harm, tethering their legal rationale to an outdated understanding of life support.
 The Supreme Court of India completely reversed this stance in March 2026. This historic judgement triggered a massive legal metamorphosis that redefined end-of-life care in the subcontinent.
The Supreme Court of India completely reversed this stance in March 2026. This historic judgement triggered a massive legal metamorphosis that redefined end-of-life care in the subcontinent.
The real breakthrough centred on the rigorous medical definition of Clinically Assisted Nutrition and Hydration (CANH). The courts had previously viewed feeding a patient as basic, undeniable human care. The old legal perspective erroneously compared tube feeding to simply offering a glass of water to a thirsty person.
The Supreme Court completely dismantled this emotional comparison. The judges ruled, with immense medical backing, that a PEG tube is a highly complex, invasive medical intervention. A Percutaneous Endoscopic Gastrostomy (PEG) tube requires surgical insertion directly through the abdominal wall into the stomach. It demands strict sterile maintenance. It necessitates continuous monitoring by trained medical professionals to prevent severe infections. It is, by every definition, artificial life support. It is absolutely not natural nourishment.
Therefore, stopping this process is entirely legally and ethically different from denying a conscious person food. Withdrawing a PEG tube is the lawful cessation of futile medical treatment.
Justices Pardiwala and Viswanathan led this profound shift. They changed the core legal standard for end-of-life care. Previous rulings always asked a purely clinical question, seeking only to know if biological life was still technically present in the body.
The new Supreme Court bench asked a profoundly human question. They asked if prolonging this biological existence was truly in the best interest of the patient. The judges applied a practical, compassionate balance-sheet approach. They weighed the heavy, painful burdens of invasive medical technology against the total lack of therapeutic benefit for Harish.
They concluded that forcing a body to function without a conscious mind offers no dignity. Refusing to prolong a vegetative state is not an act of neglect. It is a legally sound and deeply humane recognition of our biological limits.
Legal Perspective
Opines Kalyan Bhaumik, Advocate, Supreme Court of India: “The judgment as passed by the Hon’ble Supreme Court of India in the Harish Rana case accords its formal approval that the right to life encompasses the right to die with dignity. It honours the right to a dignified death over prolonged agony, free from the tyranny of futile medical interventions and artificial life support. Euthanasia (passive) for terminally ill patients is now recognised under law, as well as a Living Will (Advance Medical Directive) for patients who will eventually pass away. Just as society exists as a being, so does the law.”
The Global Journey of the Right to Die: A Timeline
The debate over human dignity and medical intervention has unfolded across continents for over fifty years. Tracing euthanasia laws by country in 2026 reveals a complex global history, where profound personal tragedies frequently became the primary catalysts for sweeping legislative reforms. From the quiet actions of a rural doctor to landmark constitutional rulings, the right to let go has been shaped by the following pivotal cases worldwide:
- 1973 (Netherlands) – Dr. Truus Postma: A rural physician administered a lethal dose of morphine to her terminally ill mother, sparking a massive public movement that ultimately laid the groundwork for the Netherlands to become the first nation to legalise euthanasia in 2002.
- 1976 (USA) – Karen Ann Quinlan: Following a devastating accident that left the 22-year-old in a persistent vegetative state, the New Jersey Supreme Court allowed her parents to withdraw her ventilator, establishing a foundational legal precedent for passive euthanasia in America.
- 1996 (Australia) – Bob Dent: Suffering from terminal cancer, Dent became the first person globally to die via legally sanctioned active euthanasia using a machine built by Dr. Philip Nitschke, though Australia’s Northern Territory law was overturned mere months later.
- 1998 (Spain) – Ramón Sampedro: The tetraplegic former seaman waged a 30-year legal battle for assisted suicide before secretly taking his own life, igniting a cultural reckoning that eventually led to Spain legalising euthanasia in 2021.
- 2011 (India) – Aruna Shanbaug: While the Supreme Court ultimately rejected the plea to end the nurse’s 42-year vegetative state, the judgement officially laid down India’s initial, foundational framework for passive euthanasia.
- 2015 (Canada) – Kay Carter & Gloria Taylor: The Supreme Court of Canada struck down the federal ban on assisted suicide in this landmark case, forcing the creation of the country’s expansive Medical Assistance in Dying (MAID) framework.
- 2026 (India) – Harish Rana: On March 11, the Supreme Court actively applied passive euthanasia guidelines for the first time, permitting the withdrawal of clinical nutrition for a 32-year-old man who had been in a persistent vegetative state for 13 years.
The Soul Beyond the Soma
Modern medicine has inadvertently created an artificial twilight zone. Technology now allows us to stretch the boundaries of physical existence far beyond natural limits. In this clinical space, death is no longer a quiet, inevitable event. It has become a heavily managed and prolonged delay. We use complex machinery to mimic the rhythms of a living body. We replace the natural drawing of breath with the mechanical click and hiss of a ventilator.
We must view this through a deeper spiritual and philosophical lens to truly understand the human cost. This perspective forces us to look beyond the heartbeat and into the essence of the individual. We must ask a fundamental question about the relationship between the soul and the soma (the body). Is the physical body merely a vessel for the human spirit? Or does it become a cage when the mind is permanently gone?
 The body usually serves as a vital vehicle for our earthly experiences and our connections to others. However, when the higher brain stops functioning permanently, that vehicle is shattered. Mercy is the courageous act of recognising when the vessel is broken beyond all repair. True compassion lies in admitting that some fragments cannot be glued back together by medical science.
The body usually serves as a vital vehicle for our earthly experiences and our connections to others. However, when the higher brain stops functioning permanently, that vehicle is shattered. Mercy is the courageous act of recognising when the vessel is broken beyond all repair. True compassion lies in admitting that some fragments cannot be glued back together by medical science.
This realisation fundamentally reframes the entire role of a physician. Medical schools teach doctors that their absolute primary duty is to heal. They are trained to fight death at every conceivable turn. But a deeper ethical understanding suggests a different responsibility. If we see death not as a failure, but as a natural, inevitable transition, then our clinical perspective shifts.
Preventing a natural departure through endless, futile intervention can become an unnatural and deeply detrimental imposition on the human body. It is not an act of care to tether a soul to a non-responsive shell for 13 years. It is, instead, a societal refusal to accept the reality of our shared mortality.
The doctor’s duty must eventually evolve from a duty to heal to a duty to release. This is not a failure of medicine; it is a profound recognition of human dignity. We must grant a patient the right to cross the final threshold without the interference of electricity, alarms, and sterile tubes. Only then can we say we are truly providing holistic care.
Beyond Borders: A Look at Euthanasia Laws by Country in 2026
India has traversed a rapid path toward legal clarity, beginning with Aruna Shanbaug in 2011, where the Supreme Court recognised passive euthanasia in principle but kept the gates tightly locked. The landmark Common Cause verdict in 2018 finally linked the right to die with dignity to the fundamental right to life under Article 21 of the Constitution.
However, the 2018 guidelines were notoriously unworkable, requiring a tedious process involving a Judicial Magistrate to countersign every Advance Medical Directive (living will). A vital update in 2023 swept these bureaucratic hurdles away, replacing mandatory magistrate approval with simple notarisation or a Gazetted Officer’s attestation. The March 2026 verdict demonstrates these streamlined rules functioning in practice, granting timely relief rather than leaving families in legal limbo.
India remains strictly committed to a passive model, allowing only the withdrawal of life-prolonging measures. This contrasts sharply with permissive European pioneers like the Netherlands and Belgium, which allow active euthanasia where a physician administers a lethal substance. Canada operates under the expansive MAID framework, sparking global debate by moving beyond terminal illness to include “grievous and irremediable” suffering.
Other nations occupy complex grey zones. The UK continues to witness fierce parliamentary debates weighing individual autonomy against the protection of vulnerable demographics. Switzerland remains a unique outlier; it lacks a codified euthanasia law, but its penal code tolerates assisted suicide provided the motive is entirely unselfish and the patient performs the final act themselves.
To ensure safety, India utilises a robust two-tier system. A Primary Medical Board of at least three specialist doctors must certify the condition is irreversible. A Secondary Medical Board, including an external nominee appointed by the Chief Medical Officer, must then concur. Under the new guidelines, these boards must provide a definitive opinion within 48 hours. This dual expert scrutiny ensures the process is medically sound, actively preventing elder abuse or hasty decisions while offering a verified path for those seeking a dignified release
The Cost of Silence: Systemic Failure
The Harish Rana case highlights a glaring, painful gap in national governance. The Supreme Court has repeatedly expressed deep frustration over legislative inaction. The Parliament has yet to codify a formal, comprehensive statutory law on euthanasia. This silence forces the judiciary to constantly step in and create complex, ad-hoc guidelines. Judges are essentially being forced to do the work of lawmakers. This lack of a clear, unified statutory framework creates lingering uncertainty for treating doctors and prolonged agony for desperate families.
 The economic reality of this legislative silence is devastating. The Rana family endured an agonizing thirteen-year emotional and financial struggle. They eventually had to sell their family home to fund over a decade of continuous intensive care. No family should ever have to trade their shelter and life savings for a biological existence that offers zero medical hope. End-of-life care must never be a privilege reserved exclusively for the wealthy. It should never become a financial curse that destroys the middle class. When the state fails to provide clear, accessible laws, it is the poor and the middle class who pay the highest price in both tears and rupees.
The economic reality of this legislative silence is devastating. The Rana family endured an agonizing thirteen-year emotional and financial struggle. They eventually had to sell their family home to fund over a decade of continuous intensive care. No family should ever have to trade their shelter and life savings for a biological existence that offers zero medical hope. End-of-life care must never be a privilege reserved exclusively for the wealthy. It should never become a financial curse that destroys the middle class. When the state fails to provide clear, accessible laws, it is the poor and the middle class who pay the highest price in both tears and rupees.
The Supreme Court directly addressed this tragedy by giving strict, uncompromising directions to the All India Institute of Medical Sciences (AIIMS). They ruled that the withdrawal of life support is absolutely not an end to care. Instead, it is a crucial transition to a different kind of care. The court mandated that the withdrawal process must be coupled with high-quality, continuous palliative care. This ensures that the patient experiences absolute zero pain or distress during their final hours.
Compassion must be highly professional and clinically precise. The medical team has a secondary, vital duty to ensure a peaceful passage. This involves expert pain management, symptom control, and deep emotional support for the grieving family standing by the bed. We must collectively move beyond the fear that turning off a machine is an act of abandonment. It is, in reality, a profound medical commitment to a painless and dignified departure.
A civilised society is not measured by how long it can keep a human heart beating using electricity and artificial pumps. It is measured by how it treats its citizens when they are at their absolute most vulnerable. We need a comprehensive parliamentary law that reflects this humanity. We can no longer afford the terrible cost of silence.
Critical Insights: The 2026 Legal Landscape
Active vs Passive Euthanasia
Passive euthanasia is legal in India and involves withdrawing life support to allow a natural death. Active euthanasia involves a physician administering a lethal dose to end suffering. This remains legal in countries like the Netherlands and Canada but is strictly illegal in India.
The Harish Rana Impact
This 2026 verdict officially reclassified feeding tubes known as Clinically Assisted Nutrition and Hydration or CANH as medical intervention. The ruling confirms that tube feeding is a technologically mediated treatment rather than basic sustenance. It empowers doctors to withdraw futile treatment for patients in a vegetative state within a swift 48 hour medical board window.
Current Status of Living Wills
In India an Advance Medical Directive is legally binding once attested by a Notary or Gazetted Officer. The 2023 and 2026 legal updates removed the requirement for a Judicial Magistrate to countersign the document. The Harish Rana case proved these directives are now actionable without months of judicial delay.
Global Leaders in 2026
India and the UK focus on passive models while other nations prioritise different degrees of patient autonomy. Canada through its Medical Assistance in Dying framework and nations like Belgium and Spain lead with active euthanasia models. Switzerland remains a distinct outlier by allowing assisted suicide as long as the assistance is not provided for selfish motives.
The Courage to Surrender
The Supreme Court anchored its historic ruling with a sentiment that resonates far beyond the marble walls of the courtroom. The judges astutely noted that while this decision can feel like a harrowing act of surrender, it is ultimately an act of profound compassion. It is a necessary admission that human wisdom and medical science have reached their absolute limits. We must eventually step aside, quiet the machines, and allow nature to take its inevitable course.
The right to die with dignity is not the opposite of the right to life. It is, in truth, the ultimate completion of it. Article 21 of the Constitution guarantees a meaningful, dignified existence. A life that is permanently reduced to a purely mechanical, unconscious process entirely lacks that protected meaning. By allowing a peaceful exit, the law fiercely protects the sanctity of the individual even in their final, quietest moments. It ensures that a person is remembered for the vibrant life they lived, rather than for the sterile machines that kept them tethered to a hospital bed for a decade.
 We return now to that quiet room where the long, agonising wait finally ends. The final threshold is no longer a place of fear, financial ruin, or legal gridlock. It is a place of profound release. As the mechanical breathing permanently stops, the biological mirror finally shatters. The artificial delay is over. This landmark ruling sets a new benchmark for euthanasia laws by country 2026 by prioritising the human spirit over clinical endurance. The heavy, unimaginable burden of thirteen years is gently lifted from the family’s shoulders.
We return now to that quiet room where the long, agonising wait finally ends. The final threshold is no longer a place of fear, financial ruin, or legal gridlock. It is a place of profound release. As the mechanical breathing permanently stops, the biological mirror finally shatters. The artificial delay is over. This landmark ruling sets a new benchmark for euthanasia laws by country 2026 by prioritising the human spirit over clinical endurance. The heavy, unimaginable burden of thirteen years is gently lifted from the family’s shoulders.
The natural journey begins at last. Harish Rana is no longer just a legal case study, a Supreme Court docket number, or a patient trapped in a permanent vegetative state. He is a human being who has finally been granted the ultimate mercy of silence. Through his legacy, we have finally learned that the greatest, most profound act of medical care is knowing exactly when to let go.